Definition
Hypertension with systemic involvement in pregnancy that develops between 20 weeks gestation and 20 weeks postpartum
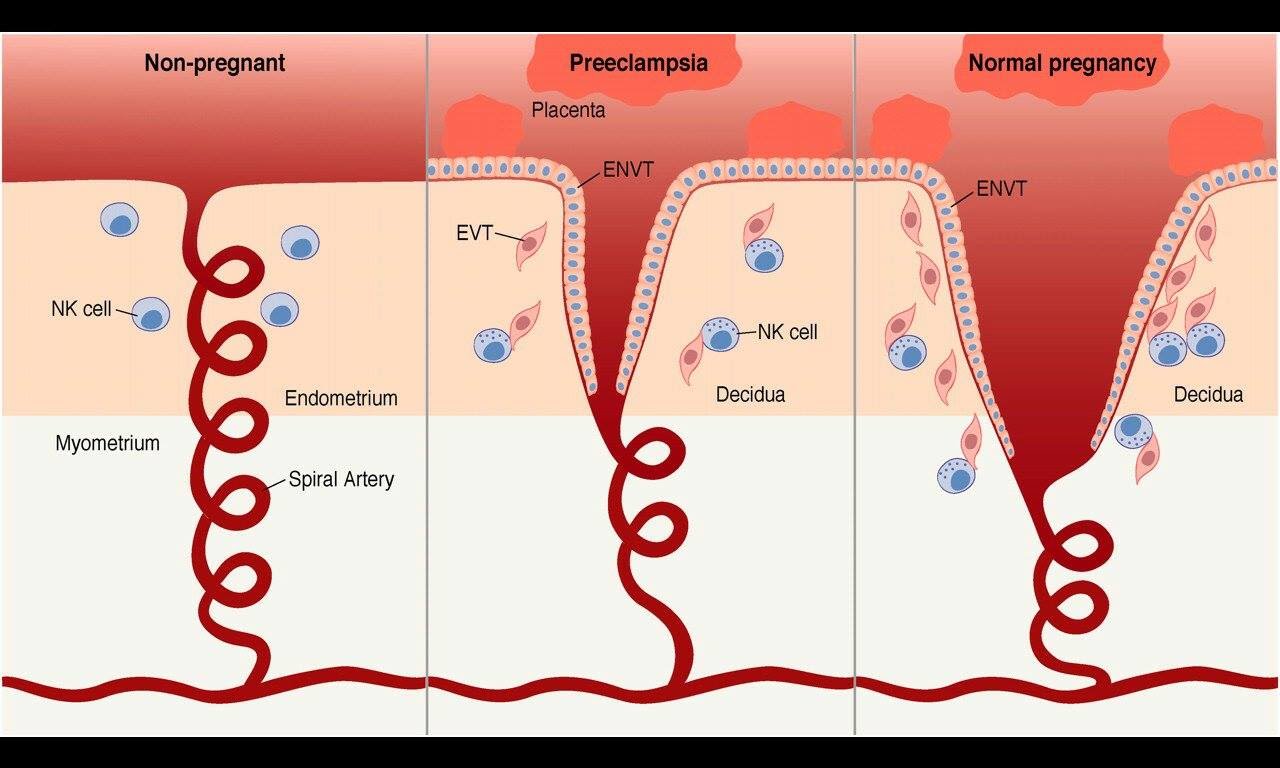
EtiologyAbnormal placentation due to failure of trophoblast invasion and incomplete spiral artery remodelling
Diagnostic criteria
- Systolic BP >140 and/or diastolic BP >90 mmHg arising after 20 weeks gestation on two or more occasions
AND
- One or more organ dysfunction
- Neurological
- Headache • Visual changes • Dizziness • Altered conscious state • Hyperreflexia • Seizure (eclampsia) • Stroke
- Haematological
- Anaemia • HELLP syndrome (haemolysis, elevated liver enzymes and low platelets)
- Hepatic
- Nausea and vomiting • RUQ or epigastric pain • Pruritis
- Renal
- Proteinuria • Oliguria • Oedema • Dyspnoea (fluid overload)
- Obstetric
- Reduced foetal movements • Intrauterine growth restriction • Placental abruption
Investigations
- Urine : protein/creatinine ratio (PCR)
- >30 mg/mmol is significant and indicates altered renal function
- Bloods
- FBE : if platelet count is low, particularly <100 x 109/L, coagulation studies are necessary
- UEC
- Serum creatinine >90 μmol/L is abnormal
- Rising serum creatinine even within normal range is a warning sign for pre-eclampsia!
- LFT
- AST >0.36 U/L indicates liver involvement
- ALP is normally elevated in pregnancy due to production by the placenta
- Urate
- Levels should approximate gestation, i.e. 0.27 mmol/L at 27/40
- Urate >0.36 mmol/L indicates renal involvement
- Blood film : may show polychromasia and schistocytes in HELLP syndrome
- Haemolytic screen : elevated bilirubin and LDH suggest haemolysis
- Imaging : foetal USS to check growth and blood flow in the umbilical cord
- Antenatal
- Hypertension : treat if systolic BP >160 and/or diastolic BP >110 mmHg
- First-line : methyldopa
- Second-line : labetalol
- Third-line : nifedipine
- Seizures : use magnesium sulphate to treat eclampsia or as prophylaxis for neurological symptoms
- Considerations for delivery
- Delivery by 37 weeks gestation is recommended to avoid progression to eclampsia
- Indications for delivery : eclampsia (when stable), uncontrolled BP despite optimal treatment, diagnosis of HELLP syndrome, abnormal renal function, placental abruption, concerns regarding foetal wellbeing
- Postnatal (signs and symptoms can continue postpartum)
- Continue treatment for 6 weeks or until resolved
- May need to follow-up with GP to repeat blood tests
- Educate regarding the risk of recurrence
- Consider the use of low-dose aspirin as prophylaxis